
Don’t worry, your back isn’t “out”

DISCLAIMER: The reader may find this blog offensive. It may stir up emotions and challenge long-standing beliefs about pain and recovery (among other things). This is intentional. The goal is behavioural change…change is hard.
As physiotherapists our clients will often come to us, speaking with sincere confidence, that their back is “out.” Despite the severity of this image, rather than looking utterly terrified, the chin is held high as they “know” why they are experiencing pain in their back. This statement is often followed by, “I know my body.”
As a therapist that emphasizes movement and function to empower clients, I will often cringe (on the inside). And to reference Game of Thrones, I think to myself:
“You know nothing, Jon Snow.”
Jokes aside, such beliefs can lead to increased pain, anxiety, and, in turn, loss of function. Sadly, this classification, that has been accurately coined as “structuralism,” most often comes from health care professionals (and physiotherapists are definitely NOT exempt from this) [1]. Before providing clear evidence as to why structuralism is a poor model (that is often harmful), let’s talk about why it is used and actually promoted by practitioners and clients alike.
Disability pays…
The more visits a therapist gets out of a client, the more lucrative it is. It’s not to say that every therapist that subscribes to structuralism is there to take your money (although some of them DEFINITELY want your money); many of these therapists truly believe in their own model.
We need to appreciate the nature of confirmation bias.
If you have been told your back is out and that you need to follow regimen “A, B, C” and attend 12x visits over the next 3 months to make your pain go away, what’s going to happen? Not surprisingly, your pain is probably going to go away. Why?
Three months have passed. Not many conditions hurt for more than three months (that’s good news!)
Placebo: you are following the recommendations because you believe it is going to work (you are committed financially, emotionally, etc): you have skin in the game. Belief in an intervention, especially when backed by finances and an “expert,” matters. The research on the placebo effect is staggering and it is far more powerful than we realize [2].
The therapist genuinely believes in what they are preaching! Given that the majority of clients improve with their “perfect” treatment, the therapist believes that their structural prescription is actually working (this is the confirmation bias in action).
Structuralism comes in many forms. We want our pain to be caused by “something.” Here are some common examples of “structural” problems:
-scoliosis
-tilted pelvis
-leg length discrepancy
-flat feet
-various joints that are “out” (back, hip, etc.)
-bulging disc(s)
-flat back
-spinal stenosis / disc degenerative disease (DDD)
-and on and on…
It’s important to recognize that there are pathologies that contribute to pain, but the pain experience should be recognized as a complex, often misleading sensation [3- more to come here; I will be putting together a pain series in the near future. If you want to watch something that helps illustrate this in entertaining fashion, check out the reference below].
Alright, with a better idea of what it is and why it’s used so extensively, let’s try to debunk “structuralism.”
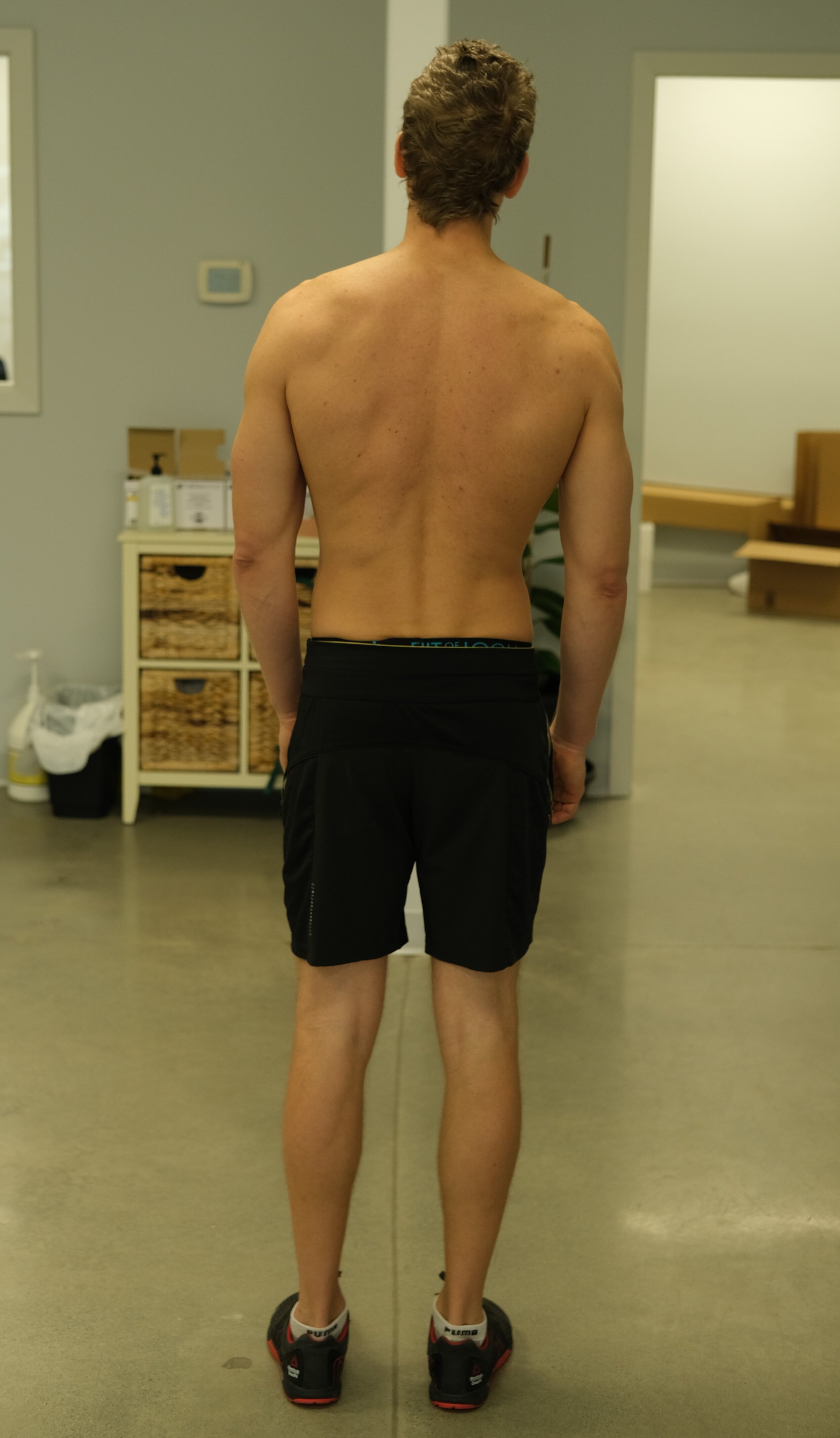
First, I want to provide insight into my own, personal experience as someone who has a somewhat “abnormal” spinal curvature (see picture below and note the deviation away from the post for reference). Despite the clear abnormality, I have had no issues of note and train hard physically seven days a week. With that structural “issue” I was able to deadlift over 400 lbs.
There is a more extreme example of an “abnormal” spinal curvature in Lamar Gant. Despite significant scoliosis (see below), he was able to lift an incredible amount of weight (661 lbs when he only weighed 132 lbs!), and was the first person to deadlift 5x his body weight.

Image courtesy of https://startingstrength.com/article/gant_bradley
A couple of people is hardly scientific and you should be pressing for more convincing evidence. Fortunately, there is a lot out there. Here are a few that should help convince you.
A study published in the British medical journal, the Lancet, way back in 1984, looked at how leg-length discrepancy related to back pain. The conclusions were quite unexpected. Leg-length differences were unrelated to back pain. Not only was there no causal relationship, but there was not even a partial correlation between leg-length discrepancy and back pain. [4]
Professionals are often concerned about the curves of the back, whether it be that it’s too extreme (“excessive lordosis” with associated pelvic tilt, hip flexor tightness, etc) or not extreme enough (“flat back” often associated with the dreaded flat-bum syndrome). A meta-analysis looking at curvature of the spine found no association between spinal curves and back pain [5].
It gets better.
Knee osteoarthritis is largely recognized and accepted as being a cause for knee pain. Almost unbelievably, a study published in 2002, found that a placebo surgery was just as good as actual arthroscopic surgery. Despite the fact that the joint was mechanically cleaned up (in the group that had the surgery), those who had a sham surgery (i.e. incisions without the arthroscopic knee clean up) recovered just as well [6].
There’s more, too…
Spinal stenosis, disc pathology, and other structural issues found on MRIs must correlate with pain, right? Not really. Often these “ugly” conditions cause no pain at all [7]. These scary sounding conditioning found on imaging are better recognized as normal findings that could be related to your pain [8].
So if “structuralism” doesn’t explain our problem, what does?
Primarily, we need to appreciate that complaints about the musculoskeletal system are more complex than “A, therefore B.” It’s much more like, “A + 2x(B+C)/D.” In other words, there are many different (important) elements that help us form a complete picture.
Given the complexity of pathologies, healthcare professionals should be collecting the pieces to help form an accurate picture. This starts with spending significant time taking a subjective history: finding out your story and exploring the elements that contribute to your unique situation (as no two situations are the same, even if the individuals had the “same” surgery). Furthermore, an understanding of pain systems (and recovery) is critical; the ability to identify when issues are more “structural” is important (and difficult!). There are times when imaging can be used to support clinical subjective/objective findings, but this is far less often than most people realize. Similarly, there are times when surgical interventions are required (but this is also far less often than most people realize!).
Finally, we need to question whether we are promoting ability or disability. The focus should be a return to function, which will almost always mean that you will be doing most of the heavy lifting (figuratively and literally). If you spend your sessions with your clinician sitting back while they make you feel good (tissue release, modalities, etc.) and you haven’t been provided movement-based exercises, you should be concerned that your “treatment” is actually promoting your disability (and not helping you get better, even if it might make you “feel” better).
We should not focus on what is “wrong” with the body. As much as we hate to admit it, we can’t tell you “exactly” what’s wrong and if someone is, your alarms should be firing (they might know nothing like Jon Snow).
A shift in perspective…
Culturally, we need to broaden our definition of “normal.” Many of us have structural differences and most of these are not problematic. Many people who are not seeking treatment for their back also have leg-length discrepancies, bulging discs, and flat backs.
Oh, and by the way, backs don’t go “out.”
References:
An excellent article on the placebo effect: https://bmjopen.bmj.com/content/5/12/e009655
TED Talk with Lorimer Moseley, “Why Things Hurt”: https://www.youtube.com/watch?v=gwd-wLdIHjs#t=8s
Grundy PF, Roberts CJ. Does unequal leg length cause back pain? A case-control study. Lancet. 1984 Aug 4;2(8397):256–8.
Christensen ST, Hartvigsen J. Spinal curves and health: a systematic critical review of the epidemiological literature dealing with associations between sagittal spinal curves and health. J Manipulative Physio Ther. 2008;31(9):690–714.
Moseley JB, O’Malley K, Petersen NJ, et al. A controlled trial of arthroscopic surgery for osteoarthritis of the knee. N Engl J Med. 2002 Jul 11;347(2):81–8.
Haig AJ, Tong HC, Yamakawa KS, et al. Spinal stenosis, back pain, or no symptoms at all? A masked study comparing radiologic and electrodiagnostic diagnoses to the clinical impression. Archives of Physical Medicine & Rehabilitation. 2006 Jul;87(7):897–903.
https://strivept.ca/2020/07/14/concerning-imaging-results-vomit/.